
The Holistic Hygiene Arm of The Dental Wellness Center
by Dr. McBride | Date Published: 2017-10-05 | Download PDF ![]()
It is agreed within all of dentistry that oral biofilm (dental plaque) is the precipitating cause of both gum disease and tooth decay. Other contributing factors that influence the effectiveness of the biofilm causing its damage are:
1. pH – relative acidity/alkalinity of saliva, which is reflective of bodily pH. Oral biofilm is much less effective in causing tooth or gum damage in a salivary environment that is neutral or slightly alkaline.
2. Excess pressure placed on teeth from an uneven bite.
3. Poor nutrition
4. Habits such as tobacco, recreational drugs or clenching/grinding teeth.
5. General health conditions, such as diabetes or metabolic syndrome.
6. Inherent genetic factors.
7. Effectiveness of daily oral self-care.
8. A person’s desire to be healthy in conjunction with #7.
9. A combination of the above factors.
Oral bacteria can’t harm the teeth and gums if they are floating within the saliva, but when they colonize in tooth-colored “clumps” on the teeth, between the teeth and gums, tongue and other areas within the mouth, they mature and evolve into a toxic mass of biofilm that injures both teeth and gums – without pain. If not removed, tooth decay will occur over time and cause a tooth ache, but rarely, if ever, a “gum ache” as gum disease isn’t painful. With gum (periodontal) disease, the bacteria within the biofilm that lies within the area between the teeth and gums (gingival sulcus) release toxic substances that actually dissolve the layer of “skin” that hugs the tooth within the sulcus, making it raw. Over time, this causes the gums to swell and injures the area of gum attachment to the tooth that deepens the sulcus, transforming it into a diseased “pocket.” During this process, the bacteria in the biofilm manufacture tartar, or calculus – a hard substance that becomes their “home.”
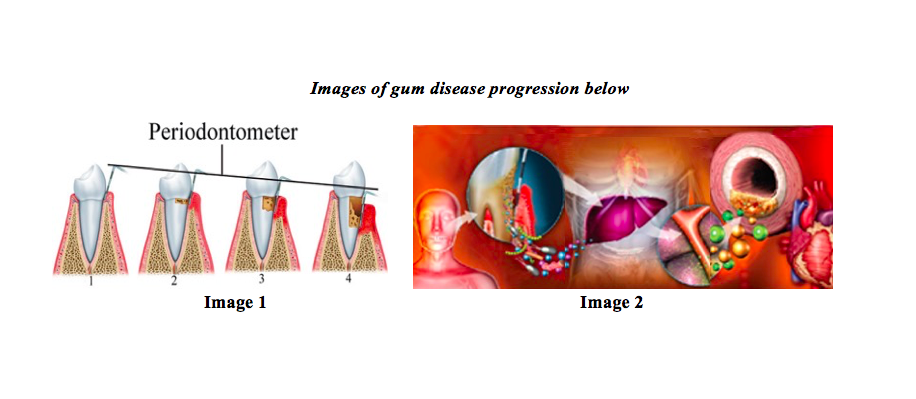
An elemental, but important diagnostic step for determining the presence of gum disease is what is known as periodontal probing, a technique taught to all dentists and hygienists while in school. During this process, the sulcus depth is measured with a sort of “dipstick” (periodontometer) that has millimeter markings. When the probe is carefully inserted to the depth of the sulcus (or pocket, if diseased), healthy depths are considered to be from one to three millimeters – with no bleeding. No bleeding would mean that the skin within the sulcus is healthy and not raw, whereas if bleeding occurs during measuring, it would indicate a loss of skin due to the toxic products caused by the bad bacteria within the biofilm. If biofilm persists within the space between the tooth and gums, it changes from a healthy sulcus to an unhealthy periodontal pocket. As time goes by, the gum tissues become infected, which:
• Causes destruction of the attachment of the gum to the tooth, deepening the pocket (Image 1).
• Destroys the supporting bone around the tooth, deepening the pocket more and eventually loosening the tooth (Image 1).
• Allows the entry of bad bacteria into the blood stream to do damage to other bodily systems (Image 2).
Is There Really a Connection Between The Mouth And The Rest of The Body?
We now have information that oral spirochetes have been found in the brains of many Alzheimer’s patients. Could these pathogenic bacteria be a factor in dementia? Another example: The March, 2013 edition of the American Heart Association Journal Circulation cites groundbreaking research showing the direct connection between oral pathogens (associated with periodontal disease and tooth decay) and acute heart attacks. It tells us that as many as half of heart attacks are being triggered by oral pathogens. Oral bacteria were found in every thrombus, and 30% had live oral pathogens in the clot!
Recent (2016) leading-edge information surfaced in a British Medical Journal showing that periodontal disease is not only associated with coronary disease, but is, in fact, a causal factor. The implications of this research are that oral bacteria can enter the bloodstream and invade the blood vessel walls. This invasion creates infections and inflammation associated with thrombi-forming events that can result in serious health issues, including heart attacks and strokes. It has been established that periodontal disease is a complex microbial and genetic disease. The most alterable factor is the microbial components of oral biofilm.
A Holistic Approach
A new patient entering the Dental Wellness Center does not have their teeth cleaned until a determination is made of the state of their gum health through a complete periodontal probing, pH testing and laboratory biofilm tests (Oravital) that show exactly the type and amount of the 8 most pathogenic bacteria found in the 600+ species of bacteria that can reside within the patients’ mouth. We have developed this approach based upon the following facts:
• A dental “cleaning” is a diagnosed procedure based upon gum pocket measurements (periodontal probing), bleeding upon measuring, and x-ray data – in other words, there are different levels of “cleanings” based upon these findings, each of which can require different appointment times – some requiring multiple appointments and more than just teeth “cleaning(s)” per below information.
• 97% of patients entering the Dental Wellness Center bleed when measured.
• Over 70% of these patients have been receiving regular cleanings.
• Half of these patients have never been measured via periodontal probing.
• Of those who have been measured, most don’t know the significance of periodontal probing.
• One in seventy new patients indicates that they have ever been properly “coached” regarding effective self-care.
• If we clean a new patient’s teeth without laboratory biofilm tests, and the patient has bad bacteria between the teeth and gums, cleaning teeth with sharp instruments will introduce them into the blood stream – not a good thing!
Information supporting the Dental Wellness Center’s mission of patient education via a thorough oral environment assessment prior to having a teeth cleaning:
1. There are over 600 species (plus their subsets) of oral bacteria, some good, and some bad. There are more bacteria inhabitants in the mouth than at the other end. This is why each new patient has a laboratory biofilm analysis to determine the bacterial types and their concentrations.
2. Phase contrast microscopic biofilm analysis offers the patient a reality as to the above by actually demonstrating to the patient what’s happening in their mouth “live, on camera.”
3. Proper coaching. Oral biofilm, the main cause of bleeding gums can be removed by patients if effectively coached.
4. Salivary pH testing. Bacteria that cause gum disease and decay thrive within an acidic oral environment (and rest of the body as well). Protocols we recommend to change it can render oral biofilm to be less harmful.
5. 90+% of dentists have contracts with dental “insurance” companies in order to be sent new patients. Dental insurance only provides benefits for cleanings and deep cleanings, not coaching/teaching time.
6. New dentists out of school, on average are over $300,000 in debt and need to provide services that have monetary benefits, therefore tempted to not “waste time” coaching patients that offers no insurance benefits.
7. During a cleaning, hygienists remove both biofilm and hard calculus/tartar – a bacterial “home” that they manufacture and live within. Calculus needs to be removed, but if the patient were coached properly with agreed-upon accountability, the calculus wouldn’t build up to the degree that it would had they not been coached – fewer patient appointments, a healthier patient both orally and systemically and a large monetary savings over time.
8. Traditionally, a “cleaning” appointment can range from one half to one hour. During this time, the hygienist is expected to thoroughly remove all of the tartar and biofilm from the patient’s teeth in a skillful, comfortable manner. This is difficult to do if a patient has unhealthy bleeding gums, and as indicated, bad bacteria may be introduced into the bloodstream. The reality is that the hygienist, for the most part, is removing the biofilm that the patient could do themselves if properly taught. In traditional, insurance-driven dental practices, if the hygienist has some time left after the cleaning, she may offer some limited home care instructions. With this scant time allotted to teaching, and with the bulk of the appointment allotted to cleaning teeth, which of the two does the patient think to be more important – the cleaning or teaching? Might it leave the patient thinking that the cleaning is of more importance for their health than the teaching about self-care? After all, they spent time in the chair and paid for a “cleaning.” This fits in with the medical sickness model, where the provider is seen as more responsible for the patient’s health than the patient.
A Health-Centered Philosophy in a Rigged Game
It all starts with the philosophy of the dentist – is the focus of the practice mainly on repairing/replacing the results of dental disease, or prevention through discovering their causes? For most all dental patients, a hygienist cannot successfully coach and properly clean teeth in a traditional one-half to one-hour allotted appointment. It is somewhat counter-intuitive as well, as the hygienist is mostly removing what the patient could themselves remove if properly coached. By their very nature, one-half to one-hour cleaning appointments deny emphasis on prevention and coaching. Might this be a reason for the burnout rate in the dental hygiene field? Teaching about causes while simultaneously treating their results is a bit oxymoronic as well – why not just teach the patient in the appointment? Because insurance pays only for cleanings, not for the time it takes for both effective coaching and a proper teeth cleaning too – and it accommodates what patients have come to know and expect from being conditioned in the past.
©2024 Robert P. McBride DDS, Inc. All Rights Reserved.